

For complete information on PCOS management, symptoms, and treatment options, read our PCOS: Complete Guide for Women
Table of Contents
TL;DR – Key Takeaways
- PCOS affects 1 in 10 women of all ages, including teenagers and young unmarried women.
- You didn’t cause it. It’s hormonal, not about lifestyle choices or relationship status.
- Early diagnosis = better outcomes. Young women have an advantage: time to manage it before fertility planning.
- It won’t stop you from having a baby when you’re ready. 70-80% of women with PCOS get pregnant with treatment.
- Get tested if: irregular periods, unexpected hair loss, persistent acne, or difficulty losing weight—even at age 16 or 20.
PCOS Doesn’t Care If You’re Married
Your best friend just told you she has PCOS. Your sister got diagnosed last month. Now you’re wondering: do you have it too?
Here’s the truth nobody talks about: PCOS affects unmarried women just as much as married women. In fact, many young women don’t realize they have it until they try to get pregnant years later.
The biggest myth? PCOS is a “married woman’s problem.” It’s not. Teenagers get it. College students get it. Single women in their 20s and 30s get it.
And honestly, getting diagnosed young is actually an advantage.
Why? Because you have years to manage it, understand your body, and get support before fertility becomes a concern.
This guide is written for young women who just got diagnosed or suspect they might have PCOS.

Why Unmarried Girls Get PCOS
It’s Not About Your Choices
First thing to know: PCOS is not caused by being unmarried, not having sex, or any relationship status. Stop blaming yourself.
PCOS develops because of a combination of genetic and hormonal factors that often show up in your teenage years or early 20s.
Genetics Play a Role
If your mother, sister, or grandmother has PCOS, your risk goes up significantly.
Your genes influence how your body handles insulin and how your ovaries produce hormones. That’s determined at birth, not by your life choices.
Insulin Resistance is Often the Root Cause
About 70% of women with PCOS have insulin resistance. This means your body doesn’t respond properly to insulin.
When insulin doesn’t work right, your ovaries produce too much androgen (male hormone). This disrupts ovulation and causes PCOS symptoms.
This can start developing in your teenage years, even before you notice any symptoms.
Inflammation in Your Body
Many young women with PCOS have chronic low-grade inflammation. Your immune system is in a constant state of activation.
This inflammation contributes to insulin resistance, hormone imbalances, and PCOS symptoms.
It’s not something you caused. It’s something your body is doing.
Gut Health Matters Too
Your gut bacteria influence your hormone metabolism and inflammation levels. If you’ve had digestive issues, antibiotics, or poor diet in your teens, your gut might be contributing.
But again: this isn’t your fault. It’s just biology.
Specific Symptoms in Young Women
Irregular or Missed Periods (The #1 Sign)
Your period used to come every 28 days. Now it’s coming every 45 days. Or it skipped two months.
For unmarried girls, this is often the first sign something’s off.
You might think it’s normal teenage variation. Sometimes it is. But if irregularity persists past age 18-20, get tested.
Heavy periods are also common. Some young women bleed for 7-10 days instead of the typical 4-5 days.
Unexpected Hair Loss (Scalp Thinning)
You’re seeing more hair in the shower than before. Your part is getting wider. You’re noticing your scalp.
This happens because excess androgens (male hormones) shrink hair follicles. It’s not about stress or your diet alone.
For young women, this can be emotionally distressing because hair is tied to appearance and confidence.
The good news? Hair regrows once you manage your hormones.
Unwanted Hair Growth (Hirsutism)
Dark hair appearing on your chin, upper lip, or stomach that wasn’t there before.
This is also androgen-related. Your body is producing male hormones that trigger hair growth in unusual places.
Again: this is medical, not something you caused.
Persistent Acne (Not Just Teenage Acne)
Everyone has acne as a teenager. But PCOS acne is different. It’s persistent, hormonal, and doesn’t respond well to typical acne treatments.
It often gets worse before your period because hormone fluctuations intensify it.
Young women with PCOS often try every acne product and get frustrated when nothing works. Spoiler: the acne won’t clear until you address the hormonal imbalance.
Weight Gain or Difficulty Losing Weight
You’re eating less than your friends, going to the gym, but the scale isn’t moving.
Insulin resistance makes weight loss extremely difficult. Your body stores fat more easily and burns it less efficiently.
This isn’t a willpower issue. It’s biochemistry.
Fatigue and Low Energy
Feeling tired all the time even when you sleep enough?
This is related to insulin resistance and hormonal imbalance. Your body isn’t efficiently converting food into energy.
Young women often attribute this to busy schedules or stress, but persistent fatigue warrants investigation.
Darkened Skin Patches (Acanthosis Nigricans)
Dark, velvety patches of skin appearing on your neck, armpits, or groin area.
This is a sign of insulin resistance. It’s not dangerous, but it indicates your body’s insulin handling is off.
Mood Changes and Anxiety
PCOS affects more than just your ovaries. The hormonal imbalance affects your brain too.
Young women report feeling more anxious, irritable, or experiencing mood swings related to their cycle.
Some experience depression or anxiety that’s more intense than typical PMS.
Difficulty Getting Pregnant (If You’ve Tried)
Some unmarried women don’t discover PCOS until they try to conceive after getting married.
If you have the symptoms above and want to conceive eventually, getting tested early gives you options and time to manage it.
Myths vs Facts About PCOS
Myth #1: “Only married women get PCOS”
FACT: PCOS affects women of all ages, including teenagers and single women. Age and relationship status have nothing to do with it.
Myth #2: “PCOS means you’re overweight”
FACT: 20-30% of women with PCOS are lean. Weight is NOT required for PCOS diagnosis.
Myth #3: “You caused PCOS by your lifestyle”
FACT: PCOS has genetic and hormonal roots. You didn’t cause it through choices.
Myth #4: “PCOS means you can’t get pregnant”
FACT: 70-80% of women with PCOS get pregnant, especially with treatment. Early diagnosis and management improve outcomes.
Myth #5: “PCOS goes away on its own in your 30s”
FACT: PCOS is a lifelong condition, but symptoms can improve with management. Getting diagnosed young helps you manage it better long-term.
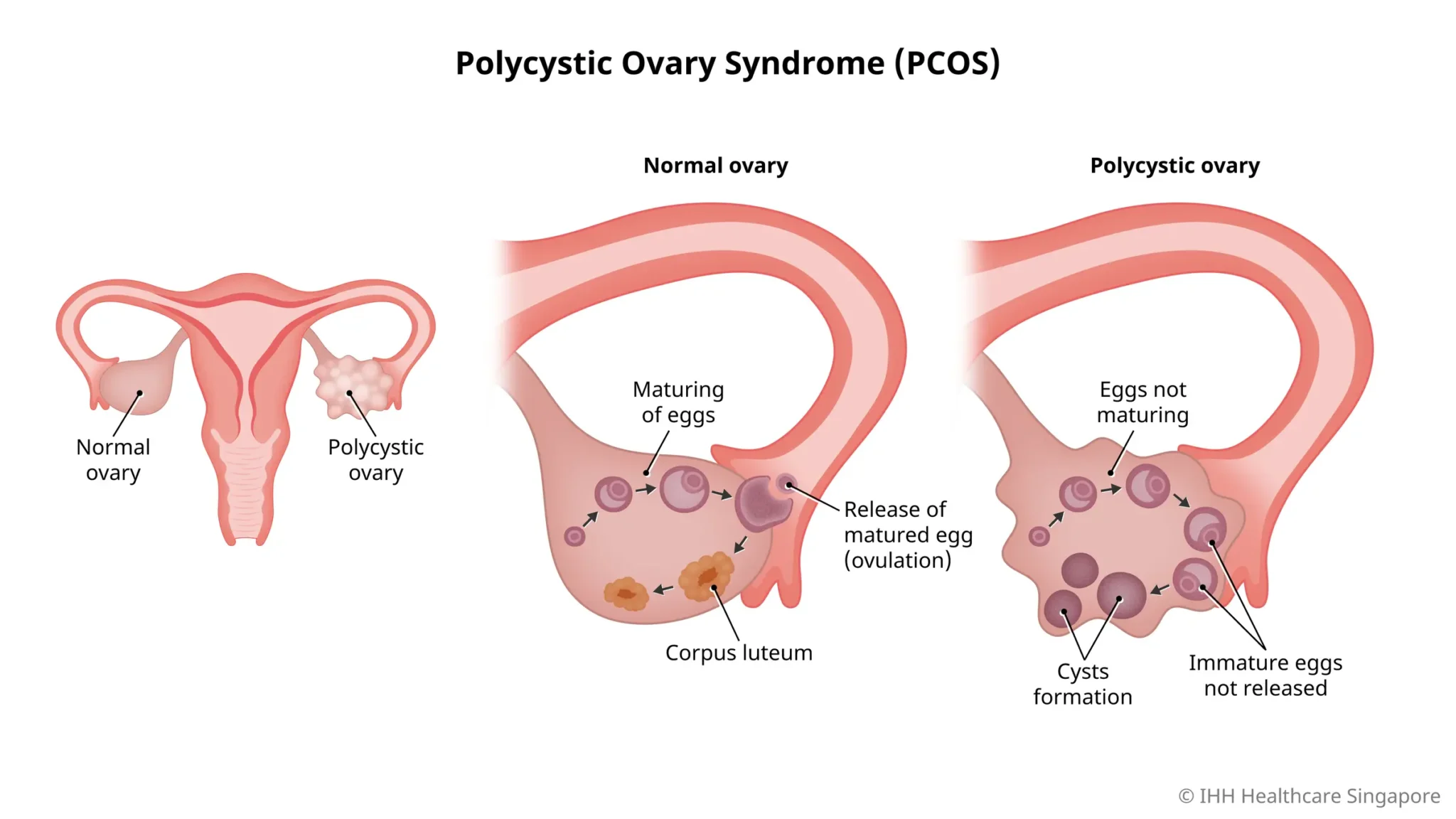
Myth #6: “If you don’t have cysts on ultrasound, you don’t have PCOS”
FACT: Diagnosis requires 2 of 3 criteria (irregular periods + high androgens + ultrasound findings). You can have PCOS without visible cysts.
Myth #7: “You should wait until you want to get pregnant to treat PCOS”
FACT: Managing PCOS now improves your quality of life today—clearer skin, better energy, easier weight management, more regular periods.
When to Get Tested {#testing}
Get Tested If You Have:
- Irregular periods (more than 35 days apart or fewer than 9 per year)
- Missed periods for 3+ months
- Unexpected hair loss or thinning
- Persistent acne that doesn’t respond to treatment
- Unwanted hair growth on face, chest, or stomach
- Difficulty losing weight despite diet and exercise
- Persistent fatigue
- Family history of PCOS
What Tests You’ll Need
Your doctor will likely order:
Blood Tests:
- Testosterone (free and total)
- LH (luteinizing hormone) and FSH (follicle-stimulating hormone)
- Fasting glucose and fasting insulin
- TSH (to rule out thyroid issues)
Pelvic Ultrasound:
- To look for polycystic ovaries
- To rule out other issues
Full Diagnosis Uses Rotterdam Criteria: You need 2 of these 3 to diagnose PCOS:
- Irregular ovulation or lack of ovulation
- High androgen levels (blood test or clinical signs like hirsutism)
- Polycystic ovaries on ultrasound
How Long Does Diagnosis Take?
Usually 2-4 weeks from initial appointment to having all test results.
Don’t rush it. A proper diagnosis requires thorough testing.
What This Means for Your Fertility
Here’s the Good News
Getting diagnosed at 20 instead of 35 is actually an advantage for fertility.
You have time to:
- Manage your hormones
- Optimize your health
- Understand your body’s fertility patterns
- Plan ahead
When You’re Ready to Conceive
70-80% of women with PCOS can get pregnant with treatment. Most don’t need IVF.
The key is getting diagnosed and managed BEFORE you try to conceive.
Women who wait until their 30s to get diagnosed often find fertility more challenging because they’ve had years of hormonal imbalance.
What You Can Do Now
Even if you’re not thinking about pregnancy:
- Get diagnosed if you suspect PCOS
- Start managing it (lifestyle, diet, possibly medication)
- Build healthy habits now
Your fertility future self will thank you.
Want more details? Read our complete guide on PCOS & Fertility: Can You Get Pregnant?
Emotional Impact & Support
This is Real
Being diagnosed with PCOS as a young woman can feel isolating. Your friends don’t have it. You might feel broken or abnormal.
You’re not. One in ten women have PCOS. You’re definitely not alone.
Feelings You Might Have
- Shame: About hair loss, acne, weight gain. This isn’t your fault.
- Anger: That your body is doing this. Completely valid.
- Anxiety: About fertility and future. But 70-80% get pregnant, remember?
- Isolation: Nobody your age talks about PCOS. But they’re experiencing it too.
- Relief: Finally having an explanation for symptoms you thought were your fault.
What Helps
- Talk to someone. A therapist, your mom, a trusted friend. PCOS is real and your feelings are valid.
- Find community. Online PCOS groups have thousands of young women going through the same thing.
- Get good medical care. A gynecologist or endocrinologist who listens and explains things.
- Remember: This is manageable. Thousands of young women manage PCOS every day.
Learn more: Read our guide on Mental Health & PCOS: The Connection Nobody Talks About
What to Do Next
Step 1: Get Diagnosed (If You Haven’t)
Book an appointment with a gynecologist or endocrinologist. Bring a list of your symptoms.
Tell them:
- Your period patterns
- Any hair changes
- Acne status
- Weight history
- Family history
Ask for: blood tests and pelvic ultrasound.
Step 2: Understand Your PCOS Type
Not all PCOS is the same. You might have:
- Hyperandrogenic PCOS (high male hormones)
- Insulin-resistant PCOS
- Inflammatory PCOS
- Lean PCOS
Understanding your type helps with treatment.
Step 3: Build Your Management Plan
For most young women, start with lifestyle:
- Regular exercise (30 minutes most days)
- Whole foods diet (avoid refined carbs)
- Stress management
- Adequate sleep (7-9 hours)
Want a detailed diet plan? Read our PCOD Diet Guide: What to Eat
Need practical tips? See our How to Control PCOD Naturally
Step 4: Be Patient
Changes take 3-6 months to show. Your hormones won’t rebalance overnight.
Stick with it. Most young women see improvements in 6 months:
- More regular periods
- Clearer skin
- Less hair loss
- Easier weight management
- More energy
Step 5: Get Support
Whether it’s a therapist, supportive friends, or an online community, don’t do this alone.
PCOS is manageable. And you’re stronger than you think.
FAQS
Q: Is PCOS contagious? Can my boyfriend catch it?
A: No. PCOS is not contagious. It’s a hormonal condition your body has. It doesn’t transfer to anyone.
Q: Will PCOS make me infertile?
A: No. PCOS makes conceiving harder, but 70-80% of women with PCOS get pregnant. Many without fertility treatment. Early diagnosis and management improve your odds.
Q: Should I tell my boyfriend/partner I have PCOS?
A: That’s your choice. Many young women do because it explains symptoms and might affect future family planning. Some prefer to keep it private until relevant.
Q: Can PCOS go away?
A: No, PCOS is lifelong. But symptoms can improve dramatically with management.
Q: Is PCOS my fault?
A: Absolutely not. PCOS is genetic and hormonal. You didn’t cause it through lifestyle choices.
Q: Will I need medication?
A: Depends on your situation. Many young women manage PCOS with lifestyle alone. Some need medication (birth control, metformin, etc.). Work with your doctor.
Q: Can I still have periods without treatment?
A: Some do, some don’t. PCOS causes irregular periods, not no periods. But medical treatment often helps regulate them.
Q: What if my doctor says it’s just stress?
A: Get a second opinion. PCOS is a medical diagnosis, not a stress-related condition. If your symptoms are persistent, you deserve proper testing.
Q: Can diet really help PCOS?
A: Yes. Diet is one of the most powerful tools for managing PCOS. Avoiding refined carbs and processed foods helps most women significantly.
The Bottom Line
PCOS is real. It’s not your fault. And you’re not alone.
One in ten women have this. Many were diagnosed young like you. They’re managing it, living normal lives, and planning futures that include pregnancy if they want it.
Your diagnosis is not your destiny. It’s just information about how your body works.
And now that you know, you can manage it.
Take action: Get diagnosed, build your management plan, and find support.
Your future self will thank you.
Eat Healthily. Stay Healthy.
Sources
- American College of Obstetricians and Gynecologists (ACOG) – PCOS Guidelines
- Rotterdam Consensus Criteria for PCOS Diagnosis
- WHO – Polycystic Ovary Syndrome Fact Sheet
- Journal of Clinical Endocrinology & Metabolism – PCOS Epidemiology
- Cleveland Clinic – PCOS in Adolescents
Links FROM this article (to other satellites):
- In Fertility section → “Learn more: PCOS & Fertility: Can You Get Pregnant?“
- In Mental Health section → “Read our guide: Mental Health & PCOS“
- In Control section → “For practical tips: How to Control PCOD Naturally“
- In Diet section → “For meal plans: PCOD Diet Guide: What to Eat“
- In Testing section → “For detailed info: PCOS Diagnosis: What Tests You Need“
